 Lung cancer
Lung cancer
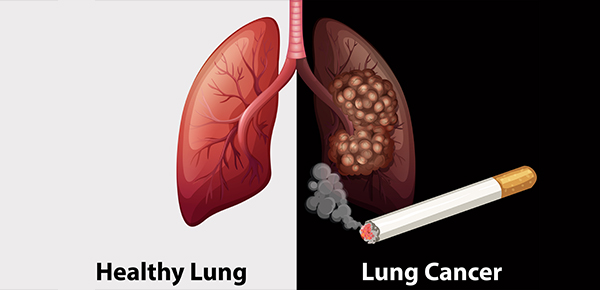
Lung cancer, also known as lung carcinoma,is a malignant lung tumor characterized by uncontrolled cell growth in tissues of the lung This growth can spread beyond the lung by the process of metastasis into nearby tissue or other parts of the body. Most cancers that start in the lung, known as primary lung cancers, are carcinomas. The two main types are small-cell lung carcinoma (SCLC) and non-small-cell lung carcinoma (NSCLC).The most common symptoms are coughing (including coughing up blood), weight loss, shortness of breath, and chest pains.
The vast majority (85%) of cases of lung cancer are due to long-term tobacco smoking.About 10–15% of cases occur in people who have never smoked.These cases are often caused by a combination of genetic factors and exposure to radon gas, asbestos, second-hand smoke, or other forms of air pollution. Lung cancer may be seen on chest radiographs and computed tomography (CT) scans. The diagnosis is confirmed by biopsy which is usually performed by bronchoscopy or CT-guidance.
Avoidance of risk factors, including smoking and air pollution, is the primary method of prevention.Treatment and long-term outcomes depend on the type of cancer, the stage (degree of spread), and the person’s overall health.Most cases are not curable.Common treatments include surgery, chemotherapy, and radiotherapy.NSCLC is sometimes treated with surgery, whereas SCLC usually responds better to chemotherapy and radiotherapy.
Worldwide in 2012, lung cancer occurred in 1.8 million people and resulted in 1.6 million deaths.This makes it the most common cause of cancer-related death in men and second most common in women after breast cancer. The most common age at diagnosis is 70 years. Overall, 17.4% of people in the United States diagnosed with lung cancer survive five years after the diagnosis,while outcomes on average are worse in the developing world.
Signs and symptoms
Signs and symptoms which may suggest lung cancer include:
- Respiratory symptoms: coughing, coughing up blood, wheezing, or shortness of breath
- Systemic symptoms: weight loss, weakness, fever, or clubbing of the fingernails
- Symptoms due to the cancer mass pressing on adjacent structures: chest pain, bone pain, superior vena cava obstruction, or difficulty swallowing
If the cancer grows in the airways, it may obstruct airflow, causing breathing difficulties. The obstruction can lead to accumulation of secretions behind the blockage, and predispose to pneumonia.
Depending on the type of tumor, paraneoplastic phenomena—symptoms not due to the local presence of cancer—may initially attract attention to the disease.In lung cancer, these phenomena may include hypercalcemia, syndrome of inappropriate antidiuretic hormone (SIADH, abnormally concentrated urine and diluted blood), ectopic ACTH production, or Lambert–Eaton myasthenic syndrome (muscle weakness due to autoantibodies). Tumors in the top of the lung, known as Pancoast tumors, may invade the local part of the sympathetic nervous system, leading to Horner’s syndrome (dropping of the eyelid and a small pupil on that side), as well as damage to the brachial plexus.
Many of the symptoms of lung cancer (poor appetite, weight loss, fever, fatigue) are not specific.In many people, the cancer has already spread beyond the original site by the time they have symptoms and seek medical attention.Symptoms that suggest the presence of metastatic disease include weight loss, bone pain and neurological symptoms (headaches, fainting, convulsions, or limb weakness). Common sites of spread include the brain, bone, adrenal glands, opposite lung, liver, pericardium, and kidneys. About 10% of people with lung cancer do not have symptoms at diagnosis; these cancers are incidentally found on routine chest radiography.
Causes


Cancer develops following genetic damage to DNA and epigenetic changes. These changes affect the normal functions of the cell, including cell proliferation, programmed cell death (apoptosis) and DNA repair. As more damage accumulates, the risk of cancer increases.
Smoking
Tobacco smoking is by far the main contributor to lung cancer.Cigarette smoke contains at least 73 known carcinogens, including benzo yrene, NNK, 1,3-butadiene and a radioactive isotope of polonium, polonium-210.Across the developed world, 90% of lung cancer deaths in men during the year 2000 were attributed to smoking (70% for women). Smoking accounts for about 85% of lung cancer cases.
Passive smoking—the inhalation of smoke from another’s smoking—is a cause of lung cancer in nonsmokers. A passive smoker can be defined as someone living or working with a smoker. Studies from the US,Europe and the UK have consistently shown a significantly increased risk among those exposed to passive smoke.Those who live with someone who smokes have a 20–30% increase in risk while those who work in an environment with secondhand smoke have a 16–19% increase in risk. Investigations of sidestream smoke suggest it is more dangerous than direct smoke.Passive smoking causes about 3,400 deaths from lung cancer each year in the USA.
Marijuana smoke contains many of the same carcinogens as those in tobacco smoke. However, the effect of smoking cannabis on lung cancer risk is not clear. A 2013 review did not find an increased risk from light to moderate use.A 2014 review found that smoking cannabis doubled the risk of lung cancer.
Radon gas
Radon is a colourless and odorless gas generated by the breakdown of radioactive radium, which in turn is the decay product of uranium, found in the Earth’s crust. The radiation decay products ionize genetic material, causing mutations that sometimes turn cancerous. Radon is the second-most common cause of lung cancer in the USA, causing about 21,000 deaths each year.The risk increases 8–16% for every 100 Bq/m³ increase in the radon concentration.Radon gas levels vary by locality and the composition of the underlying soil and rocks. About one in 15 homes in the US has radon levels above the recommended guideline of 4 picocuries per liter (pCi/l) (148 Bq/m³).
Asbestos
Asbestos can cause a variety of lung diseases, including lung cancer. Tobacco smoking and asbestos have a synergistic effect on the formation of lung cancer.In smokers who work with asbestos, the risk of lung cancer is increased 45-fold compared to the general population. Asbestos can also cause cancer of the pleura, called mesothelioma (which is different from lung cancer).
Air pollution
Outdoor air pollutants, especially chemicals released from the burning of fossil fuels, increase the risk of lung cancer. Fine particulates (PM2.5) and sulfate aerosols, which may be released in traffic exhaust fumes, are associated with slightly increased risk. For nitrogen dioxide, an incremental increase of 10 parts per billion increases the risk of lung cancer by 14%. Outdoor air pollution is estimated to account for 1–2% of lung cancers.
Tentative evidence supports an increased risk of lung cancer from indoor air pollution related to the burning of wood, charcoal, dung or crop residue for cooking and heating.Women who are exposed to indoor coal smoke have about twice the risk and a number of the by-products of burning biomass are known or suspected carcinogens. This risk affects about 2.4 billion people globally, and is believed to account for 1.5% of lung cancer deaths.
Genetics
About 8% of lung cancer is due to inherited factors. In relatives of people with lung cancer, the risk is doubled. This is likely due to a combination of genes.Polymorphisms on chromosomes 5, 6 and 15 are known to affect the risk of lung cancer.
Other causes
Numerous other substances, occupations, and environmental exposures have been linked to lung cancer. The International Agency for Research on Cancer (IARC) states there is “sufficient evidence” to show the following are carcinogenic in the lungs:
- Some metals (aluminum production, cadmium and cadmium compounds, chromium(VI) compounds, beryllium and beryllium compounds, iron and steel founding, nickel compounds, arsenic and inorganic arsenic compounds, underground hematite mining)
- Some products of combustion (incomplete combustion, coal (indoor emissions from household coal burning), coal gasification, coal-tar pitch, coke production, soot, diesel engine exhaust)
- Ionizing radiation (X-radiation, gamma radiation, plutonium)
- Some toxic gases (methyl ether (technical grade), Bis-(chloromethyl) ether, sulfur mustard, MOPP (vincristine-prednisone-nitrogen mustard-procarbazine mixture), fumes from painting)
- Rubber production and crystalline silica dust
Pathogenesis
Similar to many other cancers, lung cancer is initiated by activation of oncogenes or inactivation of tumor suppressor genes.Carcinogens cause mutations in these genes which induce the development of cancer.
Mutations in the K-ras proto-oncogene are responsible for 10–30% of lung adenocarcinomas. About 4% of non-small-cell lung carcinomas involve an EML4-ALK tyrosine kinase fusion gene.
Epigenetic changes—such as alteration of DNA methylation, histone tail modification, or microRNA regulation—may lead to inactivation of tumor suppressor genes.The epidermal growth factor receptor (EGFR) regulates cell proliferation, apoptosis, angiogenesis, and tumor invasion. Mutations and amplification of EGFR are common in non-small-cell lung carcinoma and provide the basis for treatment with EGFR-inhibitors. Her2/neu is affected less frequently. Other genes that are often mutated or amplified are c-MET, NKX2-1, LKB1, PIK3CA, and BRAF.
The cell lines of origin are not fully understood.The mechanism may involve abnormal activation of stem cells. In the proximal airways, stem cells that express keratin 5 are more likely to be affected, typically leading to squamous-cell lung carcinoma. In the middle airways, implicated stem cells include club cells and neuroepithelial cells that express club cell secretory protein. Small-cell lung carcinoma may be derived from these cell lines or neuroendocrine cells,and may express CD44.
Metastasis of lung cancer requires transition from epithelial to mesenchymal cell type. This may occur through activation of signaling pathways such as Akt/GSK3Beta, MEK-ERK, Fas, and Par6.
Diagnosis

Performing a chest radiograph is one of the first investigative steps if a person reports symptoms that may suggest lung cancer. This may reveal an obvious mass, widening of the mediastinum (suggestive of spread to lymph nodes there), atelectasis (collapse), consolidation (pneumonia) or pleural effusion. CT imaging is typically used to provide more information about the type and extent of disease. Bronchoscopy or CT-guided biopsy is often used to sample the tumor for histopathology.
Lung cancer often appears as a solitary pulmonary nodule on a chest radiograph. However, the differential diagnosis is wide. Many other diseases can also give this appearance, including metastatic cancer, hamartomas, and infectious granulomas such as tuberculosis, histoplasmosis and coccidioidomycosis. Lung cancer can also be an incidental finding, as a solitary pulmonary nodule on a chest radiograph or CT scan done for an unrelated reason.The definitive diagnosis of lung cancer is based on histological examination of the suspicious tissue in the context of the clinical and radiological features.
Clinical practice guidelines recommend frequencies for pulmonary nodule surveillance. CT imaging should not be used for longer or more frequently than indicated as extended surveillance exposes people to increased radiation.
